
 English
English  ไทย
ไทย  繁體中文
繁體中文  Português
Português  Español
Español ศูนย์หุ่นยนต์เพื่อการฟื้นฟู โรงพยาบาลบีบีเอช Robotic Center BBH Hospital
الثلاثاء, 26 نوفمبر 2019

โรงพยาบาลบีบีเอช สุขุมวิท 39 เป็นโรงพยาบาลเฉพาะทางที่ให้การดูแลผู้ป่วยที่ต้องฟื้นฟูสุขภาพโดยรับรักษาผู้ป่วยโรคหลอดเลือดสมอง ผู้ป่วยที่ได้รับบาดเจ็บที่กระดูกสันหลัง ผู้ป่วยโรคกล้ามเนื้ออ่อนแรง โรคกระดูกและข้อ และโรคที่เกี่ยวข้องกับระบบประสาทและกล้ามเนื้อผิดปรกติต่างๆ

นวัตกรรมหุ่นยนต์เพื่อการฟื้นฟู เป็นการนวัตกรรมทางการแพทย์ที่นำเทคโนโลยีหุ่นยนต์และระบบสมองกลอัจฉริยะมาใช้ในการช่วยฝึกกล้ามเนื้อเขนและขาของผู้ป่วย โดยที่ผู้ป่วยที่ไม่ต้องออกแรงพยุงตัวเอง ซึ่งสามารถใช้ได้ตั้งแต่ผู้ป่วยที่มีกำลังกล้ามเนื้อเป็นศูนย์จนถึงผู้ป่วยที่ฝึกควบคุมกล้ามเนื้อต่างๆ อุปกรณ์ที่ใช้ใน Robotic Center ของโรงพยาบาลบีบีเอช มีระบบโปรแกรมควบคุมอัจฉริยะ และระบบควบคุมโดยตรงและระบบควบคุมทางอ้อม Active & Passive mode ที่สามารถให้แพทย์และนักกายภาพบำบัดสามารถเลือกใช้ในการฝึกกล้ามเนื้อที่เหมาะสมกับผู้ป่วยแต่ละราย รวมถึงมีระบบ Bio Feedback ที่ฝึกประสาทควบคู่กันกับการฝึกกล้ามเนื้อแบบครบวงจร และรายงานผลแบบ real-time.

อุปกรณ์และเทคโนโลยีที่โรงพยาบาลบีบีเอช นำมาใช้ใน Robotic Center ได้รับการยอมรับจากผู้เชี่ยวชาญจากทั่วโลกว่าเป็นนวัตกรรมที่ดีที่สุดในปัจจุบัน มีผลการรักษาที่ดี ผู้ป่วยมีการพัฒนาได้เร็วและต่อเนื่อง ลดการบาดเจ็บในระหว่างการฝึก เป็นความหวังผู้ป่วยที่เป็นอัมพาตและครอบครัวที่จะฟื้นฟูร่างกายและพัฒนาคุณภาพชีวิตให้มีความสุขอีกครั้ง
Robotic Center ของโรงพยาบาลบีบีเอช เฟสที่ 1 ประกอบด้วย หุ่นยนต์ฝึกเดิน (Full Gait Training Robot) ที่ช่วยในการฝึกสะโพก เข่า และเท้า และ หุ่นยนต์ฝึกแขนและมือ (Hand and Arm Training Robot) ที่ช่วยในการฝึกอวัยวะท่อนบนได้แก่ ไหล่ ศอก และมือ
หุ่นยนต์ฝึกเดิน (Full Gait Training Robot)สำหรับผู้ป่วยที่มีปัญหาการเดิน รวมทั้งผู้ป่วยหลอดเลือดสมอง ผู้ป่วยที่ได้รับบาดเจ็บที่กระดูกสันหลัง ผู้ป่วยโรคกล้ามเนื้อและข้อต่างๆ ใช้ในการฝึกการเดิน ฝึกควบคุมกล้ามเนื้อและสั่งการระบบประสาท มีระบบควบคุมอัจฉริยะที่สามารถปรับความเร็วและจังหวะในการเดินให้เหมือนกับผู้ป่วยเดินด้วยตัวเอง ประกอบระบบตอบสนองอัตโนมัติ ชุดพยุงน้ำหนักที่รับน้ำหนักผู้ป่วยได้ถึง 130 กิโลกรัม และลู่เดิน ระบบออกแบบให้สามารถป้องกันอุบัติเหตุขณะฝึกได้เป็นอย่างดี
หุ่นยนต์ฝึกแขนและมือ (Hand and Arm Training Robot) สำหรับผู้ป่วยที่มีปัญหาแขน และมือ มีระบบฝึกกล้ามเนื้อแขนท่อนบน ข้อมือและนิ้วมือ มีระบบตอบสนองอัจฉริยะทั้ง 2D และ 3D ช่วยให้การฟื้นฟูได้อย่างรวดเร็ว มีประสิทธิภาพ
นอกจากนี้ศูนย์กายภาพ โรงพยาบาลบีบีเอช ยังมีนวัตกรรมการฟื้นฟูสุขภาพแบบครบวงจรด้วยเครื่องออกซิเจนบำบัด และสระว่ายน้ำเพื่อการฟื้นฟู พร้อมด้วยคณะแพทย์ที่ประกอบด้วย แพทย์ผู้เชี่ยวชาญด้านเวชศาสตร์ฟื้นฟู ศัลยแพทย์โรคกระดูกและข้อ ศัลยแพทย์โรคกระดูกสันหลัง แพทย์ผู้เชี่ยวชาญด้านระบบประสาทและสมอง รวมถึงทีมงานนักกายภาพบำบัด
เครื่องออกซิเจนบำบัด Hyperbaric Oxygen Therapy เหมาะสำหรับผู้ป่วยที่ต้องการฟื้นฟูสุขภาพและผู้ที่ต้องการเติมความสดชื่นให้แก่ร่างกาย มีประโยชน์ในการช่วยเพิ่มการไหลเวียนโลหิต เพิ่มออกซิเจนในเนื้อเยื่อ ช่วยให้บาดแผลหายไว รักษาแผลเรื้อรังที่เกิดจากเบาหวาน แผลกดทับ แผลเส้นเลือดตีบตัน และแผลที่เกิดจากการฉายรังสี ได้

สระน้ำเพื่อการฟื้นฟู Aquatic Therapy เป็นสระกายภาพบำบัดแบบปรับอุณหภูมิ ที่ออกแบบโดยเฉพาะสำหรับการออกกำลังกายและการฝึกกล้ามเนื้อ สำหรับผู้ป่วยที่มีปัญหาการเดิน การควบคุมร่างกาย เหมาะสำหรับเด็กและผู้สูงอายุ ให้ผู้ป่วยมีการพัฒนาทั้งกล้ามเนื้อและระบบประสาทได้อย่างรวดเร็ว ลดการเกิดอุบัติเหตุในขณะฝึกได้เป็นอย่างดี
แพทย์หญิงกุสุมา คุณาวงษ์กฤต ประธานเจ้าหน้าที่บริหารโรงพยาบาลบีบีเอช กล่าวว่า “การเปิดศูนย์หุ่นยนต์เพื่อการฟื้นฟู เป็นการต่อยอดและเพิ่มศักยภาพในการบริการให้กับศูนย์กายภาพของโรงพยาบาลบีบีเอช โดยคณะแพทย์และผู้เชี่ยวชาญที่ประกอบด้วยแพทย์ผู้เชี่ยวชาญด้านเวชศาสตร์ฟื้นฟู ศัลยแพทย์โรคกระดูกและข้อ ศัลยแพทย์โรคกระดูกสันหลัง และแพทย์ผู้เชี่ยวชาญด้านระบบประสาทและสมอง นักกายภาพบำบัด พร้อมให้บริการผู้ป่วยที่เคลื่อนไหวลำบาก เดินเองไม่ได้ หรือมีท่าเดินที่ไม่ถูกต้อง ผู้ป่วยโรคหลอดเลือดสมอง ผู้ป่วยไขสันหลังบาดเจ็บ เด็กสมองพิการ หรือผู้ป่วยพากินสัน โดยสามารถประเมินและวางแผนการรักษาให้กับลูกค้าได้อย่างเหมาะสม ช่วยให้ผู้ป่วยได้รับการรักษาที่สอดคล้อง ตรงกับอาการ มีผลของการรักษาที่ดีขึ้น ช่วยพัฒนาคุณภาพชีวิตของผู้ป่วยและครอบครัวให้มีความสุข”
ลูกค้าสามารถนัดหมายหรือสอบถามเพิ่มเติมได้ที่โรงพยาบาลบีบีเอช 087-494-1889 และที่ www.bbhhospital.com
- Published in News
No Comments
Wellness & Anti-aging
الإثنين, 07 أكتوبر 2019

WELLNESS AND ANTI-AGING
In this time and age of fast-paced lifestyles, emerging new stressors and pollutants, and the ever-changing healthcare needs of the 21st century, Functional Medicine offers a more practical and patient-centered approach to achieving quality of health. With an individualized and science-based practice, patients are empowered through promoting wellness and disease prevention.
Physical wellness also comes with an anti-aging benefit. Through preventive screening, health promotion through optimal nutrition, advances in biotechnology, and an understanding of each patient’s detailed genetic, biochemical, and lifestyle factors, Anti-aging solutions are identifiable and achievable.
Better Being Hospital understands and applies the principles of Functional Medicine to obtain both wellness and anti-aging.
- Published in Anti-aging & Rejuvenation Center, Services
Traumatic Brain Injury
الإثنين, 07 أكتوبر 2019

Traumatic Brain Injury
Traumatic brain injury usually results from a violent blow or jolt to the head or body. An object that penetrates brain tissue, such as a bullet or shattered piece of skull, also can cause traumatic brain injury.
Mild traumatic brain injury may affect your brain cells temporarily. More-serious traumatic brain injury can result in bruising, torn tissues, bleeding and other physical damage to the brain. These injuries can result in long-term complications or death.
Symptoms
Traumatic brain injury can have wide-ranging physical and psychological effects. Some signs or symptoms may appear immediately after the traumatic event, while others may appear days or weeks later.
Mild traumatic brain injury
The signs and symptoms of mild traumatic brain injury may include:
● Physical symptoms such as Loss of consciousness for a few seconds to a few minutes, No loss of consciousness, but a state of being dazed, confused or disoriented, Headache, Nausea or vomiting, Fatigue or drowsiness, Problems with speech, Difficulty sleeping, Sleeping more than usual, Dizziness or loss of balance
● Sensory symptoms such as Sensory problems, Sensitivity to light or sound, Cognitive or mental symptoms, Memory or concentration problems, Mood changes or mood swings, Feeling depressed or anxious
Moderate to severe tr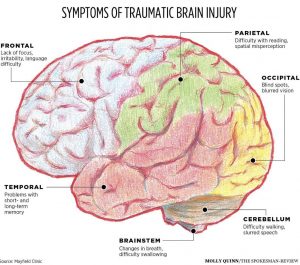 aumatic brain injuries
aumatic brain injuries
Moderate to severe traumatic brain injuries can include any of the signs and symptoms of mild injury, as well as these symptoms that may appear within the first hours to days after a head injury.
Children’s symptoms
Infants and young children with brain injuries might not be able to communicate headaches, sensory problems, confusion and similar symptoms. In a child with traumatic brain injury, you may observe change in eating or nursing habits, unusual or easy irritability, persistent crying and inability to be consoled, change in ability to pay attention, change in sleep habits, seizures, sad or depressed mood, drowsiness, loss of interest in favorite toys or activities
Causes
Traumatic brain injury is usually caused by a blow or other traumatic injury to the head or body. The degree of damage can depend on several factors, including the nature of the injury and the force of impact. Common events causing traumatic brain injury include falls, vehicle-related collisions, violence, sports injuries, explosive blasts and other combat injuries
Risk factors
The people most at risk of traumatic brain injury include:
● Children, especially newborns to 4-year-olds
● Young adults, especially those between ages 15 and 24
● Adults age 60 and older
● Males in any age group
Complications
Several complications can occur immediately or soon after a traumatic brain injury. Severe injuries increase the risk of a greater number and more-severe complications including;
● Altered consciousness
● Physical complications
● Intellectual problems
● Communication problems
● Behavioral changes
● Emotional changes
● Sensory problems
● Degenerative brain diseases
Surgical Lesions
When discussing TBI, the term “mass lesion” is often used. This refers to an area of localized injury that may cause pressure within the brain. The most common mass lesions related to TBI are hematomas and contusions. Furthermore TBI includes diffuse injuries and skull fractures.
Diagnosis
Like all trauma patients, persons with TBI need to undergo a systematic yet rapid evaluation in the emergency room. Cardiac and pulmonary function is assessed first. Next, a quick examination of the entire body is performed, followed by a complete neurological examination. The neurological examination includes an assessment utilizing the Glasgow Coma Scale (GCS). In addition to the GCS, the ability of the pupils to become smaller in bright light is also tested and also brainstem reflexes including gag and corneal (blink) may also be tested.
Radiological Tests
A computed tomography scan (CT or CAT scan) is the gold standard for the radiological assessment of a TBI patient. A CT scan is easy to perform and is an excellent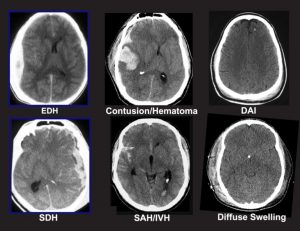 test for detecting the presence of blood and fractures, which are the most crucial lesions to identify in medical trauma cases. Plain x-rays of the skull are recommended by some as a way to evaluate patients with only mild neurological dysfunction. Magnetic resonance imaging (MRI) is not commonly used for acute head injury. However, after a patient has been stabilized, MRI may demonstrate the existence of lesions that were not detected on the CT scan. This information is generally more useful for determining prognosis than for influencing treatment.
test for detecting the presence of blood and fractures, which are the most crucial lesions to identify in medical trauma cases. Plain x-rays of the skull are recommended by some as a way to evaluate patients with only mild neurological dysfunction. Magnetic resonance imaging (MRI) is not commonly used for acute head injury. However, after a patient has been stabilized, MRI may demonstrate the existence of lesions that were not detected on the CT scan. This information is generally more useful for determining prognosis than for influencing treatment.
Surgical Treatment
Many patients with moderate or severe head injuries are taken directly from the emergency room to the operating room. In many cases, surgery is performed to remove a large hematoma or contusion that is significantly compressing the brain or raising the pressure within the skull. After surgery, these patients are usually observed and monitored in the intensive care unit (ICU).
Medical Treatment
At the present time, there is no medication or “miracle treatment” that can be given to prevent nerve damage or promote nerve healing after TBI. The primary goal in the ICU is to prevent any secondary injury to the brain. The “primary insult” refers to the initial trauma to the brain, whereas the “secondary insult” is any subsequent development that may contribute to neurological injury. For example, an injured brain is especially sensitive and vulnerable to decreases in blood pressure that might otherwise be well tolerated. One way of avoiding secondary insults is to try to maintain normal or slightly elevated blood pressure levels. Likewise, increases in ICP, decreases in blood oxygenation, increases in body temperature, increases in blood glucose and many other disturbances can potentially worsen neurological damage. The prevention of secondary insults is a major part of the ICU management of head- injured patients.
Outcome
One of the most widely used systems to classify outcome from head injury is the Glasgow Outcome Scale (GOS). Patients with mild head injury (usually defined as GCS score on admission of 13-15) tend to do well. They may experience headaches, dizziness, irritability or similar symptoms, but these gradually improve in most cases.
Patients with moderate head injuries fare less well. Approximately 60 percent will make a positive recovery, and an estimated 25 percent will be left with a moderate degree of disability. Death or a persistent vegetative state will be the outcome in about 7 to 10 percent of cases. The remainder of patients will have a severe degree of disability.
Rehabilitation
Once head-injured patients leave the acute-care hospital, some may benefit from a rehabilitation program. Prime candidates for rehabilitation are patients that had less severe initial injuries or those that have started to show significant improvement. In some cases, further recovery may be expedited by transfer to a rehabilitation hospital or to the rehabilitation service of a large hospital. For more severely injured patients or for those whose recovery is slow, constant vigilance is required to prevent the gradual onset of problems with joint mobility, skin integrity, respiratory status, infection and many other physiological functions. Patients with moderate or mild injuries, as well as severely injured patients who have improved sufficiently, may be candidates for outpatient therapy.
Prevention
To reduce the risk of brain injury you should wear a belt when driving. A small child should always sit in a child seat and install it in the back seat. Also, you should wear a helmet when riding a motorcycle, bicycle or playing sports such as skateboarding, snowmobile, or all-terrain vehicle. To protect the head in the event of an accident.
● Preventing falls can help older adults avoid falls around the house such as Install handrails in bathrooms, Put a nonslip mat in the bathtub or shower, Install handrails on both sides of staircases, Improve lighting in the home, Keep stairs and floors clear of clutter.
● Preventing head injuries in children such as Install safety gates at the top of a stairway, Keep stairs clear of clutter, Install window guards to prevent falls, Put a nonslip mat in the bathtub or shower, Use playgrounds that have shock-absorbing materials on the ground, Make sure area rugs are secure, Don’t let children play on fire escapes or balconies.
- Published in Neurological Rehabilitation Center, Services
Stroke
الإثنين, 07 أكتوبر 2019

STROKE
What is Stroke?
Stroke is a medical emergency that occurs when blood supply to the brain is interrupted or cut off due to a blockage (ischemic stroke) or a rupture of the blood vessel (hemorrhagic stroke). Bleeding and deprivation of the brain from oxygen results in brain tissue damage and brain cell death. Stroke however, can be treated and prevented.
Current diagnostic methods are highly effective and are able to identify the location of the damage or abnormalities in the brain or blood vessels, as well as any conditions and causes that could be risk factors for an impending stroke.
What are the signs and symptoms of Stroke?
- Sudden numbness or weakness on one side of the body
- Sudden confusion
- Sudden difficulty in speaking or understanding speech
- Sudden vision impairment on one or both eyes
- Sudden trouble walking, dizziness or loss of balance
- Sudden severe headache with unknown cause
What is the role of Functional Medicine in Stroke?
Stroke is highly treatable and post-stroke patients have a high chance of recovering from complications and disabilities. Functional Medicine comes in to help improve one’s symptoms through a thorough investigation, holistic rehabilitation, biochemistry work up, nutritional enhancement, supportive therapies, and other possible treatments that aid in healing the actual brain injury. Stroke may also have a tendency to recur. Because of this, Functional Medicine enables patients with the necessary preventive knowledge and measures to boost their overall health considering their identified risk factors.
- Published in Neurological Rehabilitation Center, Services


Parkinson
الإثنين, 07 أكتوبر 2019

Parkinson disease
Parkinson’s disease is a progressive nervous system disorder that affects movement. Symptoms start gradually, sometimes starting with a barely noticeable tremor in just
one hand. Tremors are common, but the disorder also commonly causes stiffness or slowing of movement.
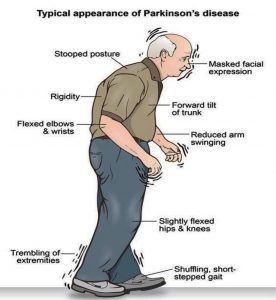
Sign and symptom
Parkinson’s signs and symptoms may include:
- Tremor, or shaking, usually begins in a limb, often your hand or fingers. You may rub your thumb and forefinger back-and-forth, known as a pill-rolling tremor.
 Your hand may tremor when it’s at rest.
Your hand may tremor when it’s at rest. - Slowed movement (bradykinesia), Over time, Parkinson’s disease may slow your movement, making simple tasks difficult and time-consuming. Your steps may become shorter when you walk. It may be difficult to get out of a chair. You may drag your feet as you try to walk.
- Rigid muscles, Muscle stiffness may occur in any part of your body. The stiff muscles can be painful and limit your range of motion.
- Impaired posture and balance, Your posture may become stooped, or you may have balance problems as a result of Parkinson’s disease.
- Loss of automatic movements, You may have a decreased ability to perform unconscious movements, including blinking, smiling or swinging your arms when you walk.
- Speech changes, You may speak softly, quickly, slur or hesitate before talking. Your speech may be more of a monotone rather than with the usual inflections.
- Writing changes, It may become hard to write, and your writing may appear small.
Causes
In Parkinson’s disease, certain nerve cells (neurons) in the brain gradually break down or die. Many of the symptoms are due to a loss of neurons that produce a chemical messenger in your brain called dopamine. When dopamine levels decrease, it causes abnormal brain activity, leading to symptoms of Parkinson’s disease. The cause of Parkinson’s disease is unknown, but several factors appear to play a role, including:
- Your genes.
- Environmental triggers.
- The presence of Lewy bodies.
- Alpha-synuclein is found within Lewy bodies.
Risk factors
Risk factors for Parkinson’s disease include:
- Age, Young adults rarely experience Parkinson’s disease. It ordinarily begins in middle or late life, and the risk increases with age. People usually develop the disease around age 60 or older.
- Heredity, Having a close relative with Parkinson’s disease increases the chances that you’ll develop the disease. However, your risks are still small unless you have many relatives in your family with Parkinson’s disease.
- Sex, Men are more likely to develop Parkinson’s disease than are women.
- Exposure to toxins. Ongoing exposure to herbicides and pesticides may slightly increase your risk of Parkinson’s disease.
Complications
Parkinson’s disease is often accompanied by these additional problems, which may be treatable: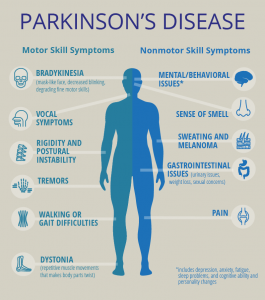
- Thinking difficulties.
- Depression and emotional changes.
- Swallowing problems.
- Chewing and eating problems.
- Sleep problems and sleep disorders.
- Bladder problems.
- Constipation.
You may also experience:
- Blood pressure changes.
- Smell dysfunction.
- Pain.
- Sexual dysfunction.
Diagnosis
A physician will initially assess for Parkinson’s disease with a careful medical history and neurological examination. People may be given levodopa, with any resulting improvement in motor impairment helping to confirm the PD diagnosis. Other causes that can secondarily produce parkinsonism are stroke and drugs.
Medical organizations have created diagnostic criteria to ease and standardize the diagnostic process, especially in the early stages of the disease. The Queen Square Brain Bank criteria require slowness of movement (bradykinesia) plus either rigidity, resting tremor, or postural instability. Other possible causes of these symptoms need to be ruled out. Finally, three or more of the following supportive features are required during onset or evolution: unilateral onset, tremor at rest, progression in time, asymmetry of motor symptoms, response to levodopa for at least five years, clinical course of at least ten years and appearance of dyskinesias induced by the intake of excessive levodopa.
Imaging
Computed tomography (CT) scans of people with PD usually appear normal. MRI has become more accurate in diagnosis of the disease which can demonstrate absence of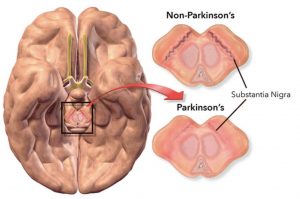 the characteristic ‘swallow tail’ imaging pattern in the dorsolateral substantia nigra. In a meta-analysis, absence of this pattern was highly sensitive and specific for the disease. Diffusion MRI has shown potential in distinguishing between PD and Parkinson plus syndromes, though its diagnostic value is still under investigation. CT and MRI are also used to rule out other diseases that can be secondary causes of parkinsonism.
the characteristic ‘swallow tail’ imaging pattern in the dorsolateral substantia nigra. In a meta-analysis, absence of this pattern was highly sensitive and specific for the disease. Diffusion MRI has shown potential in distinguishing between PD and Parkinson plus syndromes, though its diagnostic value is still under investigation. CT and MRI are also used to rule out other diseases that can be secondary causes of parkinsonism.
The metabolic activity of dopamine transporters in the basal ganglia can be directly measured with PET and SPECT scans, with the DaTSCAN. It has shown high agreement with clinical diagnoses of Parkinson’s. Reduced dopamine-related activity in the basal ganglia can help exclude drug-induced Parkinsonism. This finding is not entirely specific, however, and can be seen with both PD and Parkinson-plus disorders.
Treatment
Parkinson’s disease can’t be cured, but medications can help control your symptoms, often dramatically. In some later cases, surgery may be advised. Your doctor may also recommend lifestyle changes, especially ongoing aerobic exercise. In some cases, physical therapy that focuses on balance and stretching also is important. A speech-language pathologist may help improve your speech problems.
- Medications
Medications may help you manage problems with walking, movement and tremor. These medications increase or substitute for dopamine. People with Parkinson’s disease have low brain dopamine concentrations. However, dopamine can’t be given directly, as it can’t enter your brain. You may have significant improvement of your symptoms after beginning Parkinson’s disease treatment. Over time, however, the benefits of drugs frequently diminish or become less consistent. You can usually still control your symptoms fairly well.
- Surgical procedures
Deep brain stimulation. In deep brain stimulation (DBS), surgeons implant electrodes into a specific part of your brain. The electrodes are connected to a generator implanted in your chest near your collarbone that sends electrical pulses to your brain and may reduce your Parkinson’s disease symptoms.
- Lifestyle and home remedies
If you’ve received a diagnosis of Parkinson’s disease, you’ll need to work closely with your doctor to find a treatment plan that offers you the greatest relief from symptoms with the fewest side effects. Certain lifestyle changes also may help make living with Parkinson’s disease easier.
- Healthy eating
While no food or combination of foods has been proved to help in Parkinson’s disease, some foods may help ease some of the symptoms. For example, eating foods high in fiber and drinking an adequate amount of fluids can help prevent constipation that is common in Parkinson’s disease. A balanced diet also provides nutrients, such as omega-3 fatty acids, that might be beneficial for people with Parkinson’s disease.
- Exercise
Exercising may increase your muscle strength, flexibility and balance. Exercise can also improve your well-being and reduce depression or anxiety such as walking, swimming, gardening, dancing, water aerobics or stretching etc.
- Published in Neurological Rehabilitation Center, Services
Pain
الإثنين, 07 أكتوبر 2019

CHRONIC PAIN
Chronic pain is persistent or recurrent pain lasting longer than 3 months since onset or “pain that extends beyond the expected period of healing”. It can last long after the injury or illness that first caused it is gone. Chronic pain can last from several months to many years. It has a negative effect on a person’s well-being and ability to perform everyday activities
Pathophysiology
Under persistent activation, the transmission of pain signals to the dorsal horn may produce a pain wind-up phenomenon. This triggers changes that lower the threshold for pain signals to be transmitted. The type of nerve fibers that are believed to generate the pain signals are the C-fibers, since they have a slow conductivity and give rise to a painful sensation that persists over a long time. In chronic pain, this process is difficult to reverse or stop once established. In some cases, chronic pain can be caused by genetic factors which interfere with neuronal differentiation, leading to a permanently lowered threshold for pain.
In individuals with chronic pain, EEGs showed altered brain activity, suggesting pain-induced neuroplastic changes. More specifically, the relative beta activity (compared to the rest of the brain) was increased, the relative alpha activity was decreased, and the theta activity was diminished.
Dysfunctional dopamine management in the brain could potentially act as a shared mechanism between chronic pain, insomnia and major depressive disorder. Astrocytes, microglia, and Satellite glial cells have also been found to be dysfunctional in chronic pain. Increased activity of microglia, alterations of microglial networks, and increased production of chemokines and cytokines by microglia might aggravate chronic pain. Astrocytes have been observed to lose their ability to regulate the excitability of neurons, increasing spontaneous neural actiovity in pain circuits.
Cause
There are many possible causes of chronic pain. According to the Institute for Clinical Systems Improvement, chronic pain can be grouped into four main types.
● Neuropathic (nerve-related) pain
● Muscle pain
● Inflammatory pain
● Mechanical/compressive pain
Diagnosis
There is no way to objectively measure pain. Only the person with chronic pain can provide a description of how much pain he or she is feeling. The doctor will ask where the pain is located, how long it has been going on, and whether it is sharp or dull, constant, or occurs off and on. Sometimes a patient will be asked to rate how bad the pain is by using a numerical scale and giving more details. The doctor will do a physical exam and may order additional diagnostic tests, including
● laboratory tests to analyze blood, urine, and/or fluid from the spinal cord and brain.
● Musculoskeletal or neurological exams to assess reflexes, sensation, balance, and coordination.
● Imaging tests
○ Magnetic resonance imaging (MRI) to obtain scans of the brain, spinal cord, and other structures.
○ X-rays to obtain images of the bones, joints, and other structures.
● Electrodiagnostic procedures
○ Electromyography to test muscle activity.
○ Nerve conduction studies to record how well nerves are working.
Treatment
The for chronic pain are as diverse as the causes. From over-the-counter and prescription drugs to mind/body techniques to acupuncture, there are a lot of approaches. But when it comes to treating chronic pain, no single technique is guaranteed to produce complete pain relief. Relief may be found by using a combination of treatment options as follows;
● Drug Therapy
● Trigger Point Injections
● Surgical Implants which is rare, there are two main types of implants to control pain:
○ Intrathecal Drug Delivery.
○ Spinal Cord Stimulation Implants.
● TENS (Transcutaneous Electro-Nerve Stimulator)
● Bioelectric Therapy
● Physical Therapy
- Published in Orthopedic Rehabilitation Center, Services
Optic Nerve Atrophy
الإثنين, 07 أكتوبر 2019
- Published in Ophthalmology Rehabilitation Center, Services

